GLP-1 and Muscle Mass: What the 2025-2026 Research Actually Says

TL;DR: GLP-1 medications cause real lean-mass loss — about 25% of total weight lost on tirzepatide is lean tissue, per the SURMOUNT-1 DXA substudy (Look et al., 2025). New 2026 phenotyping data shows tirzepatide users lose 1-2% more relative lean mass than semaglutide users. The first randomized trial of resistance training in GLP-1 patients (LEAN-PREP) won't read out until 2027. Until then, the consensus from the May 2025 ACLM/ASN/OMA/TOS Joint Advisory is what we have to work with: 1.2-1.6 g/kg protein, 2-3 resistance sessions per week, and creatine if you want a supplement with non-GLP-1 evidence behind it.
We covered the basics of muscle preservation on GLP-1 medications in our original guide. That was March 2025. The research has moved since.
This is the 2026 update: what the body composition trials actually showed, why sarcopenic obesity is the signal the field is starting to worry about, and what the practical protocol now looks like with the latest evidence.
The body composition data, sorted
The first thing to get straight: yes, GLP-1 medications cause real lean-mass loss. The fight in the literature is no longer whether, but how much and whether it matters clinically.
Tirzepatide (Mounjaro / Zepbound)
The most-cited number comes from the SURMOUNT-1 DXA substudy (n=160, 72 weeks), published in Diabetes Obesity and Metabolism in February 2025 (DOI: 10.1111/dom.16275):
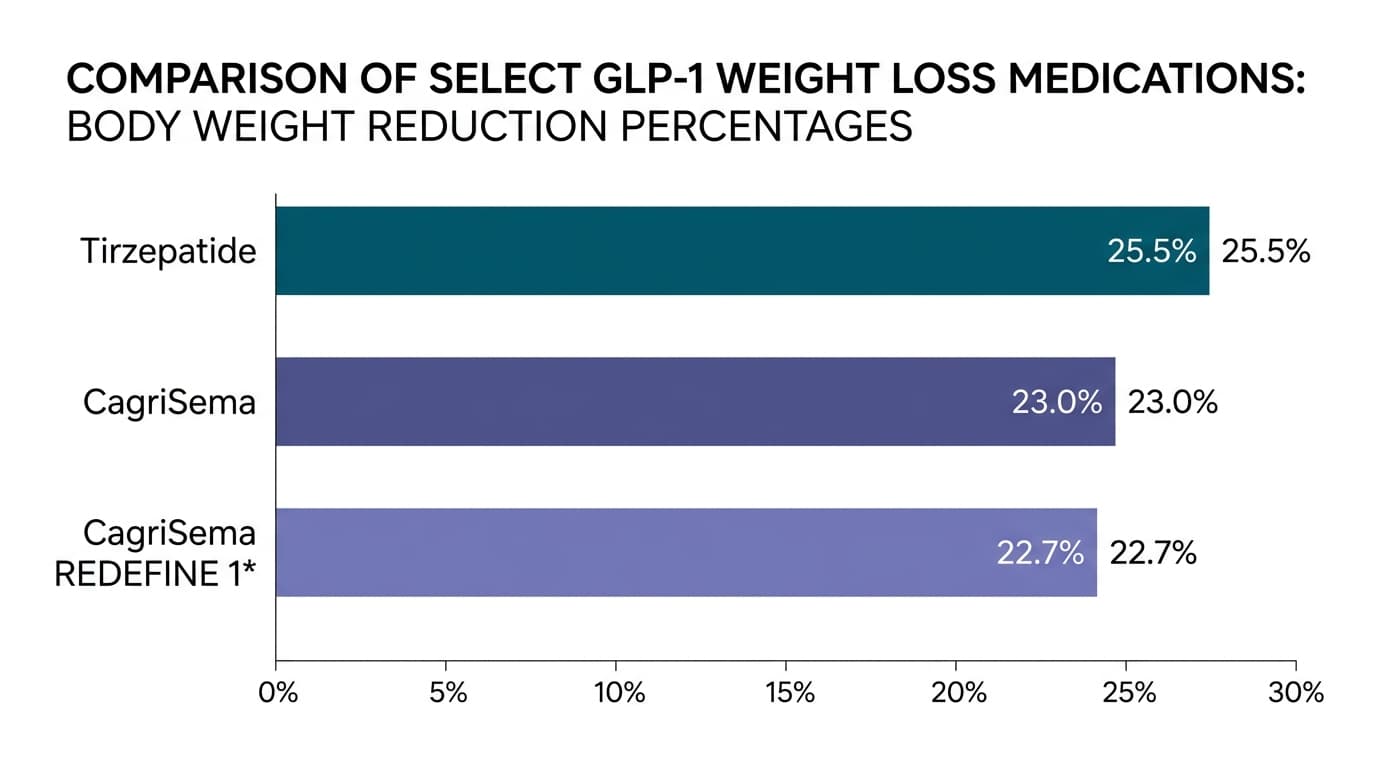
- Total weight loss: −21.3%
- Fat mass: −33.9%
- Lean mass: −10.9%
- Ratio: ~75% fat / 25% lean
In absolute terms, a 220-pound adult losing 21% of their weight on tirzepatide loses about 47 pounds total — and roughly 12 of those pounds come from lean tissue. That number gets quoted in patient forums as "you lose your muscle." It's not quite right. A meaningful portion of "lean mass" measured on DXA includes the connective tissue, organ glycogen, and intracellular water that should shrink alongside fat tissue. But it's also not nothing — a meaningful fraction is functional skeletal muscle.
Semaglutide (Ozempic / Wegovy)
The canonical reference remains the STEP 1 exploratory body composition analysis (Wilding et al., 2021, PMC8089287):
- Absolute lean mass loss: −9.7%
- Lean-mass proportion of body composition: +3.0 percentage points (the body became leaner overall)
- Lean-to-fat ratio improved by 0.23
That second line matters: even though absolute lean mass dropped, the body's overall composition shifted toward less fat per pound of lean tissue. That's the same pattern observed in intentional weight loss without medication.
The newer SEMALEAN study (n=115 with DXA, 2025, PMID 41068996) found semaglutide users lost ~3 kg of lean mass over the first 7 months — and then stabilized. The trajectory isn't a straight line down; it plateaus.
Retatrutide (next-gen, not yet approved)
Coskun et al., Lancet Diabetes & Endocrinology, June 2025 (DOI: 10.1016/S2213-8587(25)00092-0) reported the Phase 2 retatrutide body composition substudy:
- Fat mass: −26.1% at 36 weeks (8 mg dose)
- Lean-to-weight-loss ratio: "similar to other obesity treatments"
Translation: retatrutide doesn't appear to spare lean mass differently from the existing GLP-1s. More total weight loss, but the same fat:lean ratio.
Tirzepatide vs. semaglutide — the 2026 head-to-head signal
A real-world DXA phenotyping study posted to medRxiv in April 2026 (2026.04.11.26350687v1) compared body composition trajectories in tirzepatide vs. semaglutide users at 3, 6, 9, and 12 months. Tirzepatide users lost 1.1% to 2.0% more relative lean body mass than semaglutide users across all time points.
This is the first real-world signal that more aggressive weight loss (tirzepatide's edge) comes with a proportionally larger lean-mass cost. It's pre-print, not peer-reviewed yet, but the direction matches what the controlled trials already suggested.
Why sarcopenic obesity is the 2026 worry
A review published in J Nutrition, Health & Aging in August 2025 by Prokopidis, Daly, and Suetta (PMID 40819408) frames the concern bluntly: 10-20% of older adults already have sarcopenic obesity (low muscle mass with high body fat), 46-65% of GLP-1 users discontinue within 12 months, and stopping a GLP-1 is associated with about 9.69 kg of weight regain at 48-52 weeks.
The cycle the field is starting to worry about: an older adult on GLP-1 loses 12 kg total (3 kg of which is lean), stops the medication due to cost or side effects, regains 9 kg as mostly fat. They're now lighter on the scale by 3 kg but functionally weaker — they swapped 3 kg of muscle for 3 kg of fat. That is the definition of sarcopenic obesity arriving on a sharper trajectory.
This is the population — older adults, multiple medication cycles, intermittent use — where the muscle question stops being academic.
What the 2025 Joint Advisory actually recommends
In May 2025, four medical societies (American College of Lifestyle Medicine, American Society for Nutrition, Obesity Medicine Association, The Obesity Society) published a joint nutritional advisory on GLP-1 medications (Mozaffarian et al., DOI: 10.1002/oby.24336). It's the closest thing we have to consensus.
Two of the eight priorities are directly muscle-preserving:
- Adequate protein intake, distributed across meals — to support lean mass retention during energy deficit.
- Resistance training — at least 2-3 sessions per week, full body, progressive load.
The Advisory does not prescribe specific gram-per-kilogram targets. For that, we go to the existing geriatric and weight-loss literature.
How much protein, actually?
The numbers, by source:
- General healthy adults: 0.8 g/kg/day (the RDA — designed to prevent deficiency, not optimize)
- Healthy older adults: 1.0-1.2 g/kg/day (ESPEN geriatric guideline, PMID 24814383)
- Older adults at illness/malnutrition risk: 1.2-1.5 g/kg/day (ESPEN)
- Adults in active weight loss: 1.2-1.6 g/kg/day (Dietary Guidelines for Americans 2025-2030)
For a GLP-1 patient — by definition in active weight loss, often older, often eating less total food because appetite is suppressed — the target is the top of that range. Practically: 1.4-1.6 g per kg of body weight, distributed across 3-4 meals at roughly 25-40 g each.
Two refinements worth knowing:
- Per-meal threshold matters. The "muscle protein synthesis" response saturates around 25-40 g of high-quality protein per meal in older adults. Eating 100 g of protein at dinner doesn't deliver the same muscle-building signal as spreading 100 g across four meals of 25 g each.
- Use adjusted body weight if you're well above ideal weight. Calculating 1.6 g/kg on actual body weight at BMI 45 leads to unrealistic targets (200+ g). Adjusted body weight or lean body mass is the better denominator for higher-BMI patients — your dietitian can calculate it.
Resistance training: what to do without an RCT
Here's the honest disclosure: there is not yet a single completed randomized controlled trial of resistance training in GLP-1 medication users. The first one — LEAN-PREP, NCT06885736, a four-arm trial (control / resistance training / 1.6 g/kg protein / both) — has been recruiting since August 2025. The primary endpoint is quadriceps cross-sectional area on MRI. Results expected 2027.
Until then, we extrapolate from the sarcopenia-prevention literature in older adults. The protocol that has the most evidence:
- Frequency: 2-3 full-body sessions per week
- Intensity: 60-70% of one-rep max (or OMNI rated-perceived-exertion 7-8/10)
- Volume: 2-3 sets × 8-12 reps per exercise
- Exercise selection: Compound movements first (squat or leg press, hinge or row, push), accessories after
- Rest: 48-72 hours between sessions targeting the same muscle group
If you've never lifted before, start at bodyweight + a barbell or a pair of dumbbells. Progressive overload — adding load or reps each session — is the variable that matters most. The specific exercise selection matters less than consistency over 12+ weeks.
Supplements: what has evidence, what doesn't
Creatine monohydrate (3-5 g/day): Strongest non-GLP-1 evidence. Meta-analyses in older adults doing resistance training show +1.37 kg of lean tissue mass gain over training alone (PMC5679696). Zero GLP-1-specific trials, but the mechanism is independent of the medication. Take with carbs if you can; loading phase is unnecessary.
HMB (β-hydroxy β-methylbutyrate, 3 g/day): Borderline signal. A 2025 umbrella review of HMB in older adults with resistance training showed modest, statistically borderline strength gain and no consistent lean-mass effect (Bideshki et al., J Cachexia Sarcopenia Muscle, DOI: 10.1002/jcsm.13671). If your protein intake is already at 1.6 g/kg, HMB is unlikely to add much.
Leucine (the amino acid that drives MPS): Untested in GLP-1 cohorts specifically. If your protein sources are mixed (whey + meat + dairy), you're already getting plenty. Standalone leucine supplementation is not recommended absent a specific deficit.
Whey protein powder: Counts as protein, not a supplement. If you can hit your daily target with food, do that. If you can't because GLP-1-suppressed appetite makes eating 100+ g of protein from food feel like work, whey is the workaround — 25 g in a shake post-workout is the simplest path.
What this looks like in practice
If you're on a GLP-1 medication right now, the protocol is:
| Lever | Target | Source |
|---|---|---|
| Protein | 1.4-1.6 g per kg adjusted body weight, distributed across 3-4 meals of 25-40 g | ACLM/ASN/OMA/TOS Advisory 2025 + DGA 2025-2030 |
| Resistance training | 2-3 full-body sessions/wk, 60-70% 1RM, 2-3 sets × 8-12 reps | Extrapolated from sarcopenia-prevention RCTs |
| Creatine | 3-5 g/day (optional but evidence-backed) | Meta-analysis in older adults + RT |
| Cardio | 150-300 min moderate/wk (cardio doesn't preserve muscle but supports the whole system) | DGA 2025-2030 |
| Sleep | 7-9 hours; recovery is when adaptation happens | Standard sports medicine |
| Tracking | Weight + waist measurement every 2 weeks, not daily | Reduces noise, catches trend |
The single most leveraged change for most GLP-1 patients is shifting from "eat what your appetite tells you" to "hit a protein target you've written down." Suppressed appetite means it is genuinely easy to undereat protein without noticing — that's the GLP-1 trap.
Key takeaways
- Tirzepatide users lose ~25% of total weight as lean mass (SURMOUNT-1 DXA), and 1-2% more relative lean mass than semaglutide users in 2026 real-world data.
- Semaglutide lean-mass loss appears to stabilize after ~7 months (SEMALEAN, 2025).
- No RCT of resistance training in GLP-1 users exists yet. LEAN-PREP (NCT06885736) is the first; results expected 2027.
- Protein target: 1.4-1.6 g/kg adjusted body weight, distributed across 3-4 meals of 25-40 g each. Per-meal threshold matters for muscle protein synthesis in older adults.
- Creatine monohydrate (3-5 g/day) is the supplement with the strongest evidence for older adults doing resistance training. Not GLP-1-specific, but mechanism-independent.
- Sarcopenic obesity is the 2026 worry — particularly for older adults who cycle on and off GLP-1 medications.
Make the protein and the lift the part you don't skip
The medication is the easier half. The hard half is the protein target you hit on tired days and the resistance session you don't postpone in week 14. We built Gila to be the companion that makes those habits stick by structuring them around your medication phase — not a generic fitness tracker. If you'd rather assess your readiness first, take the habit readiness check.
Frequently asked questions
Do GLP-1 medications cause muscle loss? Yes — real, measurable lean-mass loss. About 25% of total weight lost on tirzepatide is lean tissue (SURMOUNT-1 DXA, 2025), and ~3 kg of lean mass lost on semaglutide over 7 months (SEMALEAN, 2025). The loss is partially preventable with protein and resistance training.
How much protein should I eat on Ozempic, Wegovy, Mounjaro, or Zepbound? The current consensus is 1.4-1.6 g per kg of adjusted body weight per day, distributed across 3-4 meals of 25-40 g of high-quality protein each. This is at the top of the standard weight-loss range, because GLP-1-suppressed appetite makes it easy to undereat without noticing.
Is muscle loss on GLP-1 medications permanent after stopping? The lean mass itself can be regained with resistance training and adequate protein after stopping. The bigger concern is the cycle: stopping a GLP-1 is associated with ~9.69 kg of regain at 48-52 weeks, mostly as fat, which can leave you with worse body composition than you started with. This is the sarcopenic-obesity trajectory the 2025 Prokopidis review highlighted.
Does tirzepatide cause more muscle loss than semaglutide? Possibly. A 2026 real-world DXA phenotyping study (medRxiv, pre-print) found tirzepatide users lost 1.1-2.0% more relative lean body mass than semaglutide users across 3-12 months. The signal is consistent with the larger total weight loss tirzepatide produces.
Can creatine prevent muscle loss on GLP-1 medications? Creatine monohydrate (3-5 g/day) has the strongest non-GLP-1 evidence for supporting lean mass gain in older adults doing resistance training (+1.37 kg meta-analytic). It hasn't been tested in GLP-1 cohorts specifically, but the mechanism is independent of the medication. It is a reasonable add to a resistance-training program.
What resistance training routine is best on GLP-1 medications? The protocol with the most evidence (extrapolated from sarcopenia prevention): 2-3 full-body sessions per week, 60-70% of one-rep max, 2-3 sets × 8-12 reps, with compound movements first. The first GLP-1-specific RCT (LEAN-PREP) reads out in 2027.
Are older adults at higher sarcopenia risk on GLP-1 medications? Yes — they enter treatment with less baseline muscle, are more vulnerable to per-meal protein synthesis thresholds, and are over-represented in discontinuation cohorts. The Aug 2025 Prokopidis review in J Nutrition, Health & Aging is the most current synthesis of this concern.
Sources
- Look M et al. SURMOUNT-1 body composition substudy. Diabetes Obes Metab, Feb 2025. DOI: 10.1111/dom.16275
- Coskun T et al. Retatrutide Phase 2 body composition. Lancet Diabetes Endocrinol, June 2025. DOI: 10.1016/S2213-8587(25)00092-0
- Wilding JPH et al. STEP 1 body composition. Diabetes Obes Metab, 2021. PMC8089287
- SEMALEAN cohort. 2025. PMID 41068996
- Tirzepatide vs semaglutide LBM phenotyping. medRxiv, April 2026 (pre-print). 2026.04.11.26350687v1
- Prokopidis K, Daly RM, Suetta C. Sarcopenic obesity in GLP-1 cohorts. J Nutr Health Aging, Aug 2025. DOI: 10.1016/j.jnha.2025.100652 (PMID 40819408)
- Mozaffarian D et al. ACLM/ASN/OMA/TOS Joint Advisory on GLP-1 Nutrition. Obesity / AJCN, 2025. DOI: 10.1002/oby.24336
- LEAN-PREP RCT protocol. Trials, 2026. NCT06885736 / PMC13110620
- Bideshki MV et al. HMB umbrella review. J Cachexia Sarcopenia Muscle, 2025. DOI: 10.1002/jcsm.13671
- ESPEN guideline on protein in older adults. Clin Nutr, 2014 (active reference). PMID 24814383
- Creatine in older adults + RT meta-analysis. PMC5679696
- US Dietary Guidelines for Americans, 2025-2030.