GLP-1 vs Intermittent Fasting: Why Stacking Them Backfires (2026 Research)
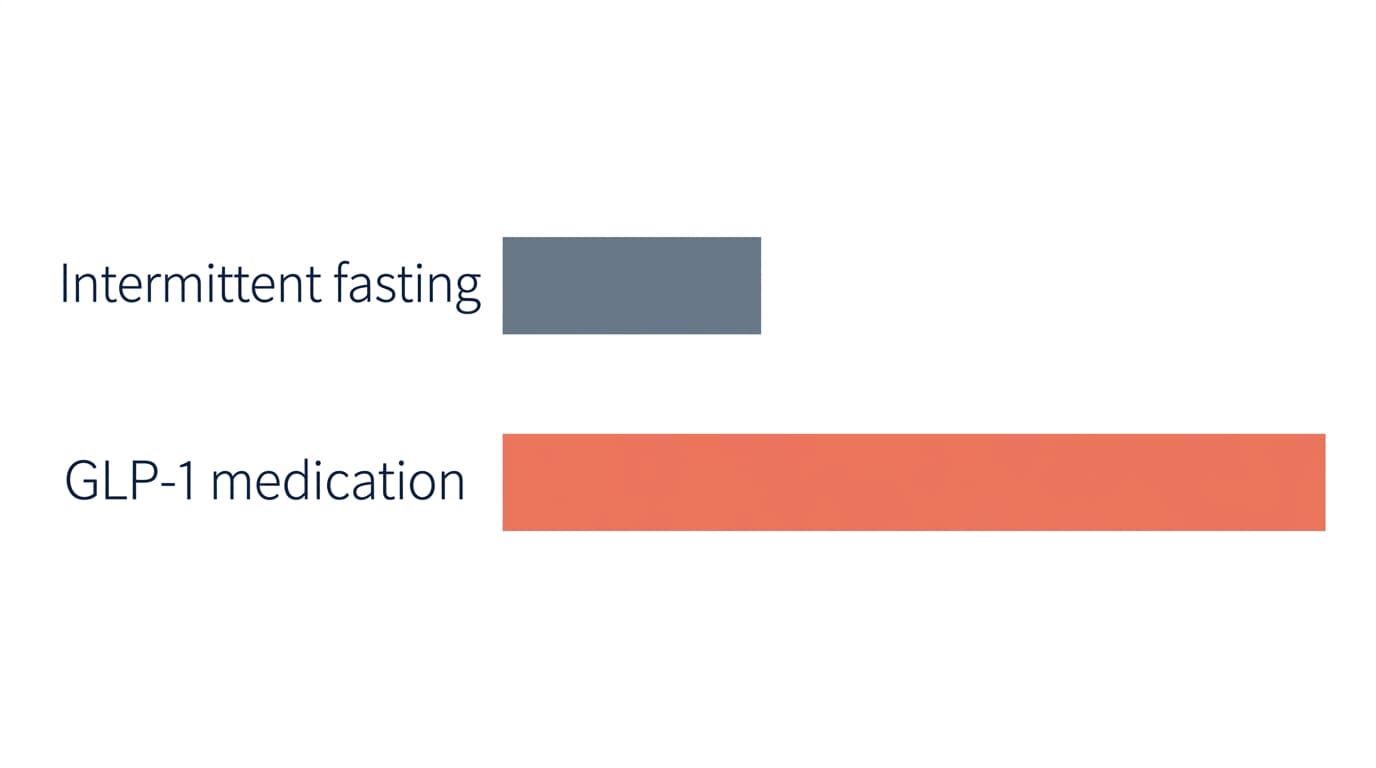
Intermittent fasting alone produces 1-3% weight loss in trials. GLP-1 medications produce 15-22%. Stacking them rarely accelerates results and often increases muscle-loss risk. Here is what the 2026 research actually shows, why the food-noise paradox matters, and what to focus on instead.
If you are on a GLP-1 medication and you've seen intermittent fasting all over social media, you have probably wondered the same thing thousands of others have asked us: should I add IF to my Ozempic, Wegovy, Mounjaro, or Zepbound routine?
It is a fair question. Both interventions promise weight loss. Both are everywhere. And the impulse to "stack" them — to make the medication work harder — is completely human.
The honest answer, based on the latest research and the mechanism of how GLP-1s actually work in your body, is: intermittent fasting on top of a GLP-1 is rarely the lever that helps, and in some cases it actively works against you. Here is what the evidence shows, and what to focus on instead.
What the latest research says about intermittent fasting alone
A 2024 New Scientist deep dive into intermittent fasting research summarized something the popular narrative has not caught up with yet: in trials of overweight and obese adults, time-restricted eating produces results that are statistically indistinguishable from doing nothing different at all. (Read the full breakdown in our companion piece on why intermittent fasting probably does not help with weight loss.)
The most rigorous trial — a 2023 randomized study published in JAMA Internal Medicine — found that limiting eating to an 8-hour window produced essentially the same weight loss as eating across a 16-hour window when total calories were matched. The fasting window itself wasn't the magic. Caloric reduction, when it happened, was.
For comparison: GLP-1 medications produce 15–22% body weight loss in clinical trials. Intermittent fasting alone in the same population produces 1–3%. They are not in the same league.
Why IF doesn't add much to a GLP-1
GLP-1 medications work by quieting hunger and food noise at the neurological level. They slow gastric emptying, increase satiety, and reduce the constant background pull toward food. Most people on a therapeutic dose are already eating less without trying, and frequently report skipping meals naturally because they're simply not hungry.
Intermittent fasting works by restricting the window in which you can eat. The mechanism is behavioral, not hormonal. When your medication is already suppressing appetite, layering an arbitrary eating window on top usually does one of two things:
- It does nothing — because you weren't going to eat in those hours anyway, so you're just naming what you were already doing.
- It compounds undereating — pushing daily calories too low, which accelerates muscle loss and slows metabolism over months.
This second risk is the one that worries clinicians most. We covered the muscle-loss problem in detail in our guide to preventing muscle loss on GLP-1 medications. Skipping breakfast on a 2.4 mg dose of Wegovy, when you are already eating 1,200 calories a day, is a fast track to losing more lean mass than you wanted.
The food-noise paradox
There is a more subtle reason intermittent fasting often disappoints people on GLP-1s: most of them came to the medication because they were exhausted by structured eating rules. The whole point of GLP-1 therapy, for many people, is the relief of not having to think about food constantly.
Adding IF puts the rules back. It re-introduces watch-checking, hunger-monitoring, and "am I allowed to eat this now?" — exactly the cognitive load that the medication just lifted. People often say the medication started feeling "less effective" once they added intermittent fasting, but what actually changed was their relationship to food. The food noise came back through the side door.
What to focus on instead
If the goal is to make your GLP-1 work better, the levers with the best evidence are not about when you eat. They are about what you eat and how you live around the medication:
- Protein, not windows. Aim for 0.8–1.0 g of protein per pound of goal body weight. Use our protein calculator if you want a starting number.
- Strength training twice a week. The single biggest predictor of preserving lean mass during GLP-1 weight loss.
- Sleep before tricks. Seven to nine hours of sleep does more for hunger regulation than any eating-window strategy.
- Consistent dose timing. Take your weekly injection on the same day, ideally the same hour. Cumulative exposure is what makes the medication work.
- Habit, not heroics. If you've hit a stall, our guide to what to do during a GLP-1 weight-loss plateau covers the small adjustments that move the needle.
When intermittent fasting might still make sense
None of this means IF is wrong for everyone on a GLP-1. There are situations where a gentler form — like a 12-hour overnight fast (essentially "stop eating after dinner") — can fit naturally, particularly:
- In long-term maintenance after tapering off your medication, when you need behavioral structure that the drug used to provide.
- For cultural or religious practices like Ramadan, where the eating window is non-negotiable. Talk to your prescriber about dose timing in this case.
- If you naturally skip breakfast and find that pattern works for your energy, mood, and lifts — but you are still hitting your protein and calorie floor.
The point is not that fasting is bad. The point is that, for most people on a therapeutic GLP-1 dose, it is a layer of complexity that doesn't earn its weight.
Key takeaways
- Intermittent fasting alone produces 1–3% weight loss in trials — far short of GLP-1 medication, which produces 15–22%.
- Adding IF on top of a GLP-1 rarely accelerates results and often increases muscle-loss risk.
- The food-noise paradox: IF reintroduces eating rules that the medication exists to remove.
- Higher-leverage moves: protein floor, strength training, sleep, consistent dose timing.
- Where IF still fits: long-term maintenance, cultural practices, or natural eating patterns — not as an accelerator.
If you are figuring out what eating pattern actually fits your medication, your body, and your life, our weekly newsletter covers the latest GLP-1 research without the hype. And if you are looking for behavior support that adapts to your stage instead of giving you another rule to follow, join the Gila pilot.
Related reading on Gila
- GLP-1 Weight Loss Statistics: The 2026 Numbers That Matter
- Retatrutide Phase 3 Results: 30% Weight Loss and the Asterisk
Related GLP-1 guides
Related Articles

Stopping and Restarting GLP-1 Is Normal — Here's What Holds the Loss
💡 **Your Journey, Your Habits!** New data from ENDO 2026 reveals that stopping and restarting GLP-1 medication is a common chapter for many, not a failure! This isn't about perfection, but about realizing that what truly anchors your weight loss through any pause are the powerful habits you build. So, let's use this window to focus on creating a sustainable foundation that outlasts any prescription!
Read more →
Moving Less on GLP-1: The Activity Drop Nobody Warns You About
A 2026 study using Fitbit data found people on GLP-1s moved less, not more — daily steps fell from 5,047 to 4,487. Here's why your body quietly slows down when you eat less, and the gentle way to protect muscle with movement and enough protein.
Read more →
GLP-1 Persistence Statistics 2026: The Start-and-Stop Numbers, Honestly
GLP-1 persistence statistics for 2026, read honestly: how many people stop (about 4 in 10 in year one), how many restart (most of them), why they pause, and the behavior layer that separates regain from kept loss. Every figure linked to a primary source.
Read more →Ready to start your GLP-1 journey?
Gila helps you build lasting habits, understand your body, and stay on track. Join the pilot for free.
Join the Pilot